Athanasios Papadis, MD; Ilias Kosmas, MD; Ioannis Iakovou, MD, PhD; Jacob Doll, MD, FSCAI
Introduction
Vascular access is a necessary clinical skill in interventional cardiology. Common vascular access procedures include central venous and peripheral arterial cannulation. Success depends on patient anatomy, comorbid conditions, and operator skill. Ultrasound (US) guidance for vascular access has been in clinical practice for more than 30 years. Several studies demonstrate increased safety, effectiveness, and efficiency of US-guided vascular access as compared to access by only utilizing anatomical landmarks. Despite the existing evidence, US-guided femoral access for coronary and structural percutaneous interventions (PCIs) has not been widely adopted. Surveys of interventional cardiologists demonstrated that only 13% to 27% of operators routinely use US guidance for femoral access. Consensus documents have classified US-guided vascular access of the internal jugular vein, femoral vein, and femoral artery as 1B recommendations. For radial access, the evidence is less extensive. Whilst US guidance did not demonstrate a benefit in clinical outcomes compared with the standard (SD) palpation technique, it improved the efficiency and overall success rate of arterial access. All operators easily mastered transradial access and US guidance techniques.
In this Tip of the Month, we highlight practical aspects of US guidance for vascular access in the field of interventional cardiology, focusing mainly on femoral artery and vein, radial artery, and internal jugular vein.
US Imaging Views
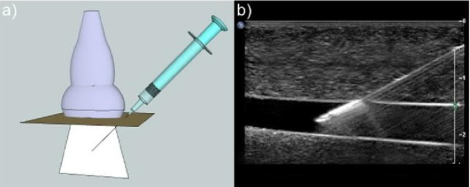
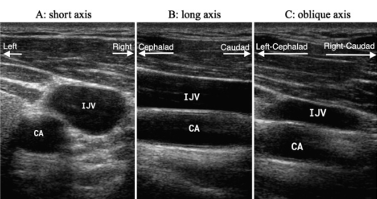
Long-axis view (LAX) (longitudinal view): The plane of the probe is parallel to the LAX of the vessel. The entire length and the tip of the needle can be seen, as well as the depth of insertion, thereby avoiding insertion of the needle beyond the target vessel. It is technically challenging in part that the needle and US beam should be perfectly aligned.
Short-axis view (SAX) (transverse view): The plane of the probe is perpendicular to the vessel. It allows us to view the artery and vein simultaneously, as well as the surrounding structures and their relative positions to the needle. Identification of both vascular structures is paramount; it may be easier to direct the cannulating needle toward the target vessel and coincidentally away from surrounding structures. There is faster cannulation time with SAX compared with the LAX approach, and the novice operators perceived the SAX approach as easier to use than the LAX approach. The drawback of this method is that the entire length or tip of the needle cannot be visualized.
Oblique-axis (OAX) view: OAX is obtained by initially locating the vessel in the SAX, followed by rotation of the probe to almost midway between the SAX and LAX. It may allow better visualization of the needle shaft and tip and offers the safety of imaging surrounding structures in the same view, thus capitalizing on the strengths of both the SAX and LAX approaches.
Needle Visualization
US scanning is used to verify the presence and position of a suitable target vessel before skin puncture, and real-time US imaging is used to guide the needle tip into the vessel.
There are two approaches:
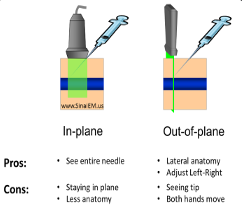
- In-plane approach: Regardless of the vessel view, the whole shaft of the needle is getting visualized as it progresses toward the target.
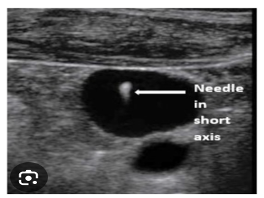
- Out-of-plane approach: The needle is advanced perpendicular to the transducer beam, providing a SAX of the needle(hyperechoic dot).
US-Guided Access
Below is a stepwise approach to US-guided access:
- Preprocedural US evaluation of the vessel
- Recognition of possible local disease
- US-guided real-time puncture
- Verification of the direction of guidewires and catheters into the vessel
- Detection of possible postprocedural complications
Access Site-Specific Details, Recommendations, and Tips
- US-guided vascular access of the internal jugular vein
- This reduces overall complications and time to cannulate, as well as improves first-time success (1B).
- In terms of safety and efficacy, the out-of-plane approach is similar to the in-plane approach (2A).
- US-guided access of the femoral vein
- This reduces major complications and time to successful cannulation, as well as improves the success rate (1C.)
- This also decreases infectious and thrombotic complications (e.g., hematoma) (1C).
- An out-of-plane puncture using a SAX is recommended (1C).
- US-guided cannulation of radial artery
- For all hypotensive, hypovolemic and hemodynamically unstable patients, vascular diseases, and small arteries, this reduces complications, the time to successful cannulation, and the number of attempts (1B).
- The SAX out-of-plane approach is not superior to the LAX in-plane approach (2A).
- The SAX out-of-plane approach is superior to the LAX in-plane approach.
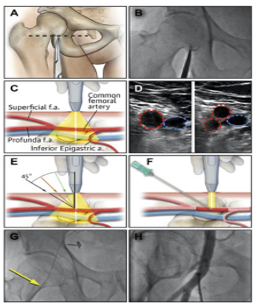
- US-guided access of femoral artery during elective procedures
- This reduces complications and time to cannulation, as well as increases both overall success and first-time success rates (1B).
- The planned puncture area is at the common femoral artery, above the bifurcation of the superficial and profunda femoral arteries, at the level of the femoral head.
- Areas of vessel wall calcification or luminal stenosis should be avoided.
- The presence of a femoral artery pulse should be checked before the procedure.
- Fluoroscopy of the femoral head can further assist.
Summary
With the increasing use of large-bore sheaths and the parallel technical improvements of US-guided techniques, the need for US guidance of vascular access is increasingly relevant. The importance of proper training for achieving competency in US-guided access must be emphasized.
References
- Lamperti M, Bodenham AR, Pittiruti M, et al. International evidence-based recommendations on ultrasound-guided vascular access. Intensive Care Med. 2012 Jul;38(7):1105–1117.
- Reusz G, Csomos A. The role of ultrasound guidance for vascular access. Curr Opin Anaesthesiol. 2015 Dec;28(6):710–6.
- Lamperti M., Biasucci DG, Disma N, et al. European Society of Anaesthesiology guidelines on peri-operative use of ultrasound-guided for vascular access (PERSEUS vascular access) Eur J Anaesthesiol. 2020 May;37(5):344–376.
- Xenogiannis I, Varlamos C, Keeble TR, et al. Ultrasound-Guided Femoral Vascular Access for Percutaneous Coronary and Structural Interventions. Diagnostics (Basel).2023 Jun 11;13(12):2028.
- Sandoval Y, Burke MN, Lobo AS, et al. Contemporary Arterial Access in the Cardiac Catheterization Laboratory. JACC Cardiovasc Interv. 2017 Nov 27;10(2):2233–2241.
- Lamperti et al. Eur J Anaesthesiol 2020; 37:344–376 Guidelines for Performing Ultrasound
- Nguyen P, Makris A, Hennessy A, et al. Standard versus ultrasound-guided radial and femoral access in coronary angiography and intervention (SURF): a randomised controlled trial. Eurointervention. 2019 Aug9;15(6):e522–e530.
- Troianos CA, Hartman GS, Glas KE, et al. Guidelines for Performing Ultrasound Guided Vascular Cannulation: Recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. JASE. 2011 Dec;24(12):P1291–1318.
- “Ultrasound Courses-CME-Registry Review-Gulfcoast Ultrasound Institute.” Www.gcus.com, Gulfcoast Ultrasound Institute, www.gcus.com/.
Related QI Tips
Other evidence-based methods and tools you can use to improve quality of care and outcomes for patients.