Talla A. Rousan, MD, FSCAI; Konstantinos Dean Boudoulas, MD, FSCAI; Jayant Bagai, MD, FSCAI
Introduction
Transcatheter aortic valve replacement (TAVR) has evolved over the past decade with advancement in sheath delivery and valve technology. On occasion, interventional cardiologists may still encounter difficulty in delivering the transcatheter heart valve (THV) due to challenging anatomy, including horizontal heart and tortuous aorta. This can lead to increased procedure time and the potential for complications. In this Tip of the Month, we focus on a few strategies that can be used to overcome these challenges when performed via transfemoral access.
Strategies to overcome challenging anatomic scenarios include the following:
TAVR in a horizontal heart (for both self-expandable and balloon-expandable valves):
- A multidetector computed tomography (MDCT) measures the aortic angle, which is defined as the angle between the horizontal and aortic annular planes in the coronal section. An angle of 48°or more defines a horizontal heart.1 Patients with an aorto-ventricular angle over 70° are more challenging and were originally excluded from the self-expandable TAVR clinical trials2 (see Figure 1). In addition, severe unfolding and marked tortuosity (hyperacute bend) of the thoracic aorta were excluded from the balloon expandable TAVR clinical trial in high-risk patients.3
- The buddy balloon technique can be used to facilitate the advancement of the THV across the native valve.4 Steps include the following:
- Advance an additional stiff wire to the aortic root.
- Use a peripheral balloon as a “shoehorn” to allow the valve to slide over it and facilitate its delivery across the aortic valve.
- The loop snare technique can be used.5 Steps include the following (see Figure 2):
- Perform this technique with the THV in the ascending aorta.
- Use the contralateral femoral artery access (8F sheath) to advance a nitinol hydrophilic wire (e.g., 0.018-inch 300 cm Radifocus wire, Terumo Corp., Tokyo, Japan) to the ascending aorta through a 4F IM catheter.
- Remove the 4F IM catheter.
- Advance a gooseneck snare through the 8F sheath; snare the distal tip of the hydrophilic wire in the ascending aorta; and make a loop around the THV above the crimped valve (see Figure 1).
- Externalize the snared end of the hydrophilic wire.
- Advance an 8F JR4 guide catheter over both ends of the externalized hydrophilic wire and advance the guide catheter to the ascending aorta while cinching a loop around the nose cone or the body of the THV delivery system above the crimped valve.
- Have one operator advance the valve across the native aortic valve, while the other operator pulls on the loop snare to make the position and alignment more favorable.
- Once the THV crosses the native valve, remove the JR4 guide catheter and hydrophilic wire if looped to the nose cone prior to THV deployment.
- In some cases of extreme horizonal heart and thoracoabdominal aorta tortuosity, it may be challenging to cross the aortic valve and advance the stiff wire into a safe position in the left ventricular (LV) apex. In these cases, advance a 90 cm sheath through the TAVR sheath into the ascending aorta, then use a 120 cm JR4 catheter to cross the valve and advance it into the LV cavity. Following that, replace the JR4 catheter with pigtail catheter, then advance a stiff wire to the LV apex per the usual fashion (see Figure 3).
TAVR in tortuous aorta:
- There are no clear objective parameters to define aortic tortuosity. Severe angulations and calcification of the thoracoabdominal aorta may prolong the procedure and make it more challenging; however, it has not been clearly associated with increased risk of complications.6
- The double wire technique can be used to straighten the aorta and facilitate delivery of the valve system.7 Steps include the following:
- Use two Lunderquist wires (Cook Medical, Bloomington, Indiana).
- Advance one wire into the LV cavity and the second wire through a catheter (e.g., multipurpose) into the proximal ascending aorta.
- Remove the wire and catheter located in the ascending aorta once the THV is advanced across the aortic valve.
- For a severe S-shaped aorta, the triple stiff wire technique can be used.4 Steps include the following:
- Use three Lunderquist
- Advance one wire into the LV cavity and advance two wires through an 8F guide catheter (e.g., multipurpose or Amplatz) into the proximal ascending aorta.
- Remove the wires and guide catheter located in the ascending aorta once the THV is across the aortic valve.
Summary
In this Tip of the Month, we described different strategies to advance the THV across the aortic valve in challenging anatomic scenarios. Operators can use different techniques and innovate to safely cross the aortic valve in these cases and should carefully review the MDCT and other pertinent imaging for proper procedural planning. When difficulties delivering the THV from the femoral access persist despite using the tips detailed above, operators should consider an alternative access.
References
- Abramowitz Y, Maeno Y, Chakravarty T, et al. Aortic Angulation Attenuates Procedural Success Following Self-Expandable But Not Balloon-Expandable TAVR. JACC Cardiovasc Imaging. 2016 Aug;9(8):964–72.
- Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014 May 8;370(19):1790–8.
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011 Jun 9;364(23):2187–98.
- Noble S, Roffi M. Retrograde aortic valve crossing of the CoreValve prosthesis using the buddy balloon technique. Catheter Cardiovasc Interv. 2014 Nov 15;84(6):897–9.
- Naganuma T, Kawamoto H, Hirokazu O, et al. Successful use of the loop snare technique for crossing a degenerated surgical valve with the Evolut-R system. Catheter Cardiovasc Interv. 2019 Jun 1;93(7):E400–E402.
- Toggweiler S, Leipsic J, Binder RK, et al. Management of vascular access in transcatheter aortic valve replacement: part 2: Vascular complications. JACC Cardiovasc Interv. 2013 Aug;6(8):767–76.
- Buzzatti N, Mangieri A, Cota L, et al. Use of double stiff wire allows successful transfemoral transcatheter aortic valve implantation through extreme thoracic aorta tortuosity. Circ Cardiovasc Interv. 2015 Apr;8(4):e002331.
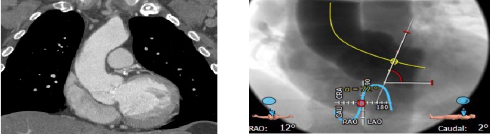
Figure 1. CT angiography showing a horizontal heart with an aortoventricuar angle over 70°.
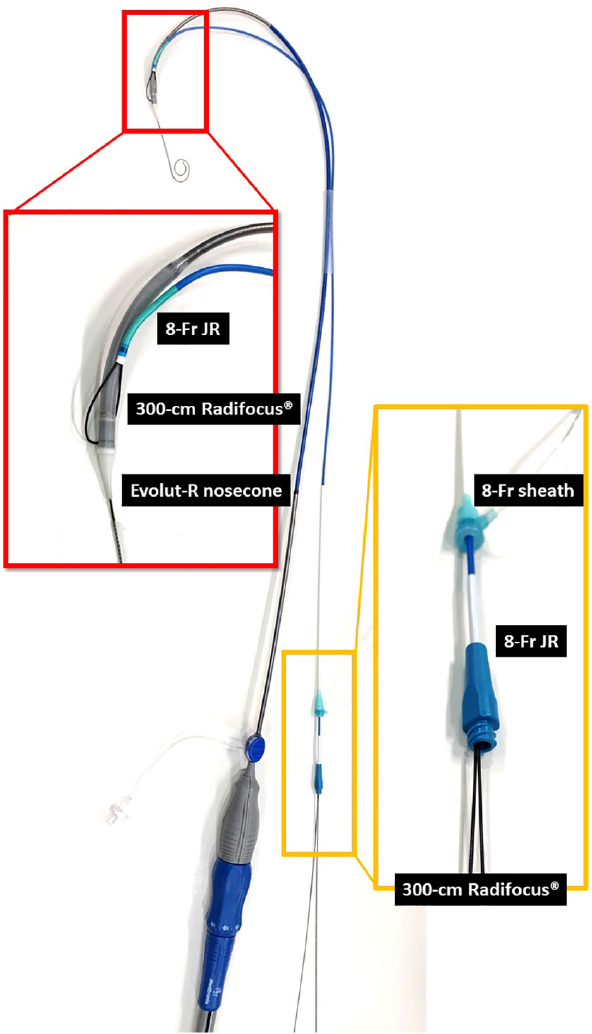
Figure 2. The loop-snare technique5.

Figure 3. Using a 90 cm sheath (arrow head) to facilitate crossing the aortic valve.
Related QI Tips
Other evidence-based methods and tools you can use to improve quality of care and outcomes for patients.