Introduction
As the field of interventional cardiology continues to expand, highlighted by the emergence of several transcatheter structural interventions, the common femoral artery (CFA) and common femoral vein (CFV) will be increasingly accessed(1). Operator technique determines safety of the arteriotomy and effectiveness of closure following procedure completion. It is for these reasons that it is essential we identify patients’ anatomical risk profile while obtaining access to facilitate large bore structural interventions. The success of any structural intervention accessing either the CFA or CVA relies heavily on excellent access technique. This article provides an overview of contemporary best practices for obtaining safe large-bore percutaneous transfemoral access during transcatheter structural heart interventions.
Anatomy
A thorough understanding of the anatomy is essential when accessing the femoral vasculature. The CFA arises from the external iliac artery (EIA) and is defined as starting inferior to the inguinal ligament and ending at the bifurcation of the superficial femoral artery (SFA) and the deep femoral artery (DFA) (profunda femoris)(2)(Figure 1). The inferior epigastric artery (IEA) courses around the inguinal ligament and aids in identifying the location of the inguinal ligament angiographically(2). The ideal location of arterial puncture is within the zone of the CFA, below the IEA, above the bifurcation and directly on the femoral head. An arteriotomy’s proximity to the femoral head allows for direct manual compression against a bony structure if needed for hemostasis. Arterial puncture above the IEA risks retroperitoneal bleeding due to location preventing manual compression for hemostasis and thus must be avoided(3,4). Arterial puncture distal to the bifurcation of the CFA risks arteriotomy of smaller vessels, and increases potential for complications such as pseudoaneurysm formation(3,5).
Access Technique
Surface Anatomy:
Prior to the widespread use of imaging techniques including fluoroscopy and ultrasound to identify vascular structures, palpation and landmark identification were utilized for vascular access. The inguinal ligament connects the anterior superior iliac spine with the pubic symphysis and thus can be palpated in between these two structures. Just inferior to the inguinal ligament is the femoral triangle, which includes (from medial to lateral) the femoral vein, common femoral artery, and the femoral nerve. The common femoral artery bifurcates and further gives off the deep femoral artery. The inguinal crease was commonly used as a reference point for the femoral triangle, however this method has been shown to be unreliable in relation to the anatomy of the femoral artery(2). Once the inguinal ligament is identified by palpation, the provider then palpates for the strongest femoral pulse below this landmark. The needle trajectory should be angled with intent to puncture approximately 1-2 centimeters below the inguinal ligament. Risks of “blind” puncture include difficulty of identifying the inguinal ligament (especially in obese patients), variable trajectory of the needle, and anatomic variants or pathology such as high bifurcation, plaque, and calcification(3).
Fluoroscopy:
Fluoroscopy allows for visualization of the bony structures of the patient. By fluoroscopy, the ideal location of the puncture is within the mid third of the femoral head. Under fluoroscopy, the provider can place a tool (i.e. covered needle, hemostat) over the patient near the possible target and visualize the location of the femoral head in relation to the tool. This ensures that the arteriotomy is made in the region of the femoral head, which becomes advantageous in applying manual pressure for hemostasis against a bony structure. Additionally, once access is obtained, the provider can perform angiography of the femoral artery to identify the location of arteriotomy and location of the femoral artery bifurcation. Fluoroscopy also assists in identification of calcifications within the vasculature. Calcified areas should be avoided as puncture of a calcified segment may prevent optimal hemostasis.
Ultrasound Guidance:
Importantly, ultrasound allows for identification of the CFA bifurcation, location of the CFV and thus increases accuracy of obtaining an anterior wall stick in arterial puncture within the target zone (Figure 2). Use of ultrasound also provides the benefit of direct visualization while inserting the access needle, reducing both time-to-access as well as number of attempts(6). As previously mentioned, it is best to avoid puncture in a calcified area as this can prevent proper hemostasis; ultrasound guidance aids in visualization of calcified vessel walls. As a supplement to ultrasound, palpation of the femoral artery and surrounding structures as well as fluoroscopy assist in optimal puncture. There is robust evidence to support the routine use of ultrasound when obtaining access, which for large bore procedures such as structural interventions can decrease the risk of vascular complication as well as increase the success of both obtaining access and safe hemostasis following the conclusion and removal of large-bore sheaths(6,7).
Micropuncture Technique:
Use of a micropuncture needle and subsequently a micropuncture sheath, prior to upsizing of the catheter to large-bore, is an additional step that can be taken to ensure safe arteriotomy. This involves puncture of the femoral artery under ultrasound guidance with a micropuncture needle (21 gauge, compared to the traditional 18 gauge needle) and insertion through this needle with the micropuncture guidewire. After which, anterior-posterior fluoroscopy can confirm location of the arteriotomy on the femoral head (Figure 2). Once this has been confirmed, a micropuncture sheath can be introduced into the CFA through which angiography can be performed to confirm that it is above the bifurcation and below the IEA (Figure 2). If the arteriotomy site is not optimal, the introducer sheath can be removed and manual pressure for 1-2 minutes applied with ability to reattempt. If the arteriotomy is well positioned, the introducer sheath can be exchanged over guidewire with larger-bore sheaths and eventual large-bore sheath intended for use of the structural intervention. With the use of micropuncture access, arterial puncture and access is limited to a small bore catheter, allowing for adjustment if needed and may mitigate access site complications(8).
Conclusion
The ongoing success and expansion of transcatheter structural heart interventions will continue to rely heavily on appropriate and careful contemporary technique when obtaining femoral arterial access. The micropuncture ultrasound-guided technique can result in precise arteriotomy insuring avoidance of plaque and important branches, ultimately increasing the likelihood of safe and successful femoral access during structural heart interventions.
References
- Otto CM, Nishimura RA, Bonow RO et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021;143:e35-e71.
- Swift H, Bordoni B. Anatomy, Bony Pelvis and Lower Limb: Femoral Artery. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Bruno Bordoni declares no relevant financial relationships with ineligible companies., 2024.
- Bangalore S, Bhatt DL. Femoral arterial access and closure. Circulation 2011;124:e147-56.
- Kawamura A, Piemonte TC, Nesto RW, Gossman DE. Retroperitoneal hemorrhage from inferior epigastric artery: value of femoral angiography for detection and management. Catheter Cardiovasc Interv 2006;68:267-70.
- Tulla K, Kowalski A, Qaja E. Femoral Artery Pseudoaneurysm. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Andrew Kowalski declares no relevant financial relationships with ineligible companies. Disclosure: Erion Qaja declares no relevant financial relationships with ineligible companies., 2024.
- Jolly SS, AlRashidi S, d'Entremont MA et al. Routine Ultrasonography Guidance for Femoral Vascular Access for Cardiac Procedures: The UNIVERSAL Randomized Clinical Trial. JAMA Cardiol 2022;7:1110-1118.
- Rashid MK, Sahami N, Singh K, Winter J, Sheth T, Jolly SS. Ultrasound Guidance in Femoral Artery Catheterization: A Systematic Review and a Meta-Analysis of Randomized Controlled Trials. J Invasive Cardiol 2019;31:E192-E198.
- Ben-Dor I, Sharma A, Rogers T et al. Micropuncture technique for femoral access is associated with lower vascular complications compared to standard needle. Catheter Cardiovasc Interv 2021;97:1379-1385.
Figure 1:
Femoral arterial anatomy with the ideal target site of arteriotomy being above the bifurcation and below the inferior epigastric artery on the femoral head.
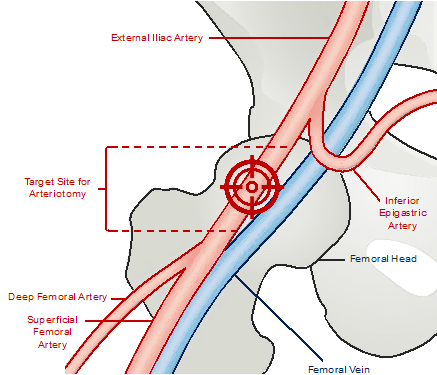
Figure 2:
All authors: Mehak Kapoor, DO, and Giorgio Medranda, MD, FSCAI
Other Specialist Resources for Structural Heart Disease
Including recently published studies, coverage of late-breaking science, updates from clinical trials and registries, and complex case presentations.